Agency
Agency is simply the ability of an individual to make their own choices and act accordingly. Having agency means having a sense of self, particular values and cultural identity, and being able to pursue self-determined goals through strategic action. A sense of agency tells you that you can make a difference in the world and that it’s your responsibility to do so. It supports independent thinking and encourages people to seek innovative solutions to problems they encounter.
Through agency, people devise ways of adapting flexibly to remarkably diverse geographic, climatic and social environments; they figure out ways to circumvent physical and environmental constraints, redesign and construct environments to their liking… By these inventive means, people improve their odds in the fitness survival game.
- Albert Bandura
Mental flexibility
Our perception of the world isn’t how it really is. It’s an interpretation based upon our previous experience, developmental history, culture and evolution. This is why we all experience the world differently, even if we are in the same room or even the same conversation. Our brain develops these mental models of how the world works because of the need for efficiency. There are far too many inputs from all our senses, much redundant information, and any alternative would quickly lead to cognitive overload. The resultant mental moment that we experience is based upon perceived relevance. Our brain is always trying to make unpredictable circumstances predictable.
When I was training to be an obstetrician, I came across women who declined medical input into high-risk pregnancies, who chose to home birth or free birth (with no trained attendant) despite the obvious risk to the life of themselves or their baby. These experiences were incompatible with how I understood the world. But of course my understanding was based upon the experience of an educated male who had been through the standard course of medical training. My mental models were limited. I took the opportunity to read texts about home birth and to hear why women choose this option. I read the online discussion forums and came to understand a new perspective. This didn’t always change my advice when I reencountered similar situations, but it gave me an understanding of motivations, the ability to empathise and a language to help me engage more genuinely in shared decision-making options.
Mental flexibility in response to VUCA
In a VUCA environment, prior mental models and predictions are a poor guide for the future. A healthy response would be to adjust the weighting of our previous assumptions, guided by feedback from the environment. This feedback is acquired through usual methods but in particular active listening and curiosity. We would then act and update our mental models accordingly.
An individual’s response to uncertainty is determined by several factors, such as prior experiences, our state of mind - e.g. stress, boredom, fatigue - and environmental context, for example, if we feel under threat. Also, people who are less anxious about change, unpredictability, and conflicting mental models will naturally perform better in changing environments.
Uncertain environments lead to arousal, and the biological response of arousal frees up cognitive resources in preparation for the adaptive change outlined above. If this doesn’t occur, long term arousal is harmful and leads to reduced performance as well as diseases such as high blood pressure, depression and suppression of our immune system. The stress many have experienced in response to the challenge of COVID-19 is testament to this.
Cognitive biases
If an individual is unable or unwilling to respond adaptively to uncertainty, they often succumb to cognitive biases and ‘sculpt and select’ sensory inputs to be more consistent with established mental models and predictions. Without self-awareness and mental flexibility, outdated models can lead to poor decision-making that is out of touch with the current world. Sometimes people respond to uncertainty with rigid frameworks to maintain a sense of control and decrease their own anxiety. Trying to avoid uncertainty isn’t a good long-term strategy in the modern world.
Humans, however, can be very adaptive to change, with high intrinsic motivation to deal with uncertainty and to learn the skills to manage unpredictable situations. These are the skills we need to teach and nurture in our students. Adapting mental flexibility is challenging, but it isn’t impossible.
Meta-learning
Unfortunately, learned skills have a limited short-life in a changing environment, so the ability and drive to learn continuously is the only solution for success. Meta-learning is defined as ‘...being aware and taking control of one’s own learning’ (Biggs J, 1985). This includes the principles and strategies that make learning more efficient, including retrieval practise, spacing, interleaving, feedback, elaboration and testing. Self-regulated learning leads to a valuable sense of agency and improvements in academic outcomes and life success.
Learning and self-efficacy
From an educational perspective, it’s essential to recognise that agency is enhanced when learners appreciate that shortfalls in achievement are primarily due to things they can do something about, rather than an underlying lack of capacity to learn. Humans cannot avoid difficulties such as failure, criticism and inequity, nor can we avoid the usual emotions that go with them: disappointment, anxiety and fear. Those who have previously experienced the ability to rise above setbacks will be more able to see themselves doing so once again. Enabling students to experience success will contribute positively to meta-cognitive skills and personal sense of agency.
Summary
It is very unlikely that the VUCA norm of the modern world is going to change anytime soon. The attributes of enhanced agency, mental flexibility and having the knowledge and motivation to continually learn will provide a foundation for lifelong success whatever career or path is chosen.
Recommended resources
Systems Thinking - Russell Ackoff
This presentation from 2015 remains a fascinating critique of modern-day educational approach and discusses the importance of motivation, agency and meta-learning.
‘Your future depends upon your capacity to learn and your motivation to do so’
‘ Teaching is an obstruction to learning’
‘In school we kill creativity. Examinations encourage students to think about what examiners expect. To provide known answers. This systematically kills creativity.’
Link to video
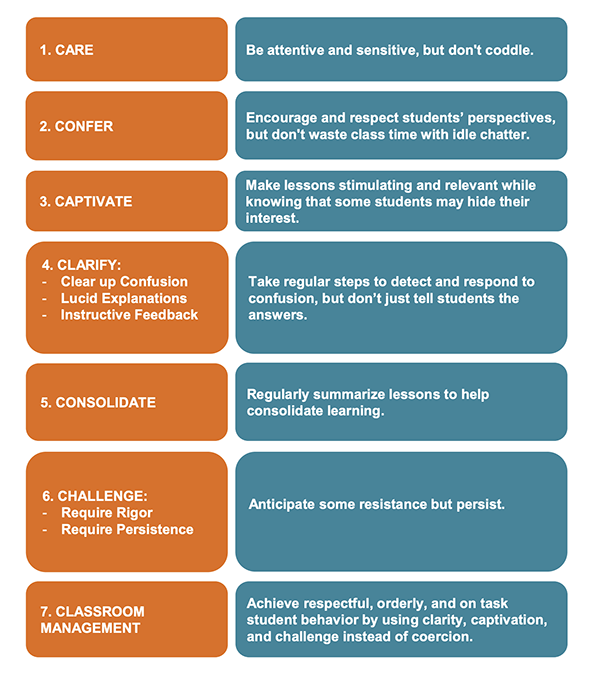
Encouraging agency in others
The influence of teaching: beyond standardised test scores: Engagement, Mindsets and Agency. A summary of the practical steps to help students develop agency is listed from page 10.